
Frozen Shoulder: Psychosocial & Hormonal Influences — Evidence Review
- Adrian Wildborne

- Apr 14
- 7 min read
Updated: May 5
Frozen shoulder (adhesive capsulitis) has long been viewed as a purely local inflammatory and fibrotic shoulder problem. Newer research instead suggests that frozen shoulder sits at the intersection of hormonal, neuroendocrine, metabolic and psychosocial systems, rather than being just a structural joint issue.
This article summarises key evidence on how stress, mood, hormones and metabolism interact with the shoulder capsule and may shape onset, severity and recovery.

Hormonal Factors
Oestrogen Deficiency and Menopause

Frozen shoulder is more frequent in women aged 40–60, with outpatient data indicating a female-to-male ratio of around 2:1. This sex disparity has directed attention towards oestrogen.
Post-menopausal women not receiving hormone replacement therapy (HRT) appear to have higher odds of developing adhesive capsulitis than those on HRT, in large observational cohorts.
Clinical trials are now underway to explore whether HRT may modify frozen shoulder outcomes when combined with standard care.
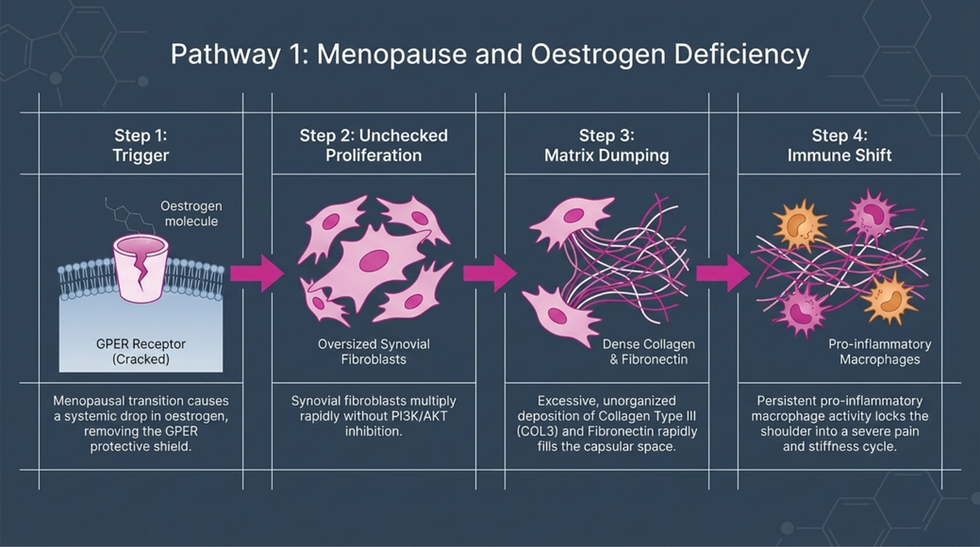
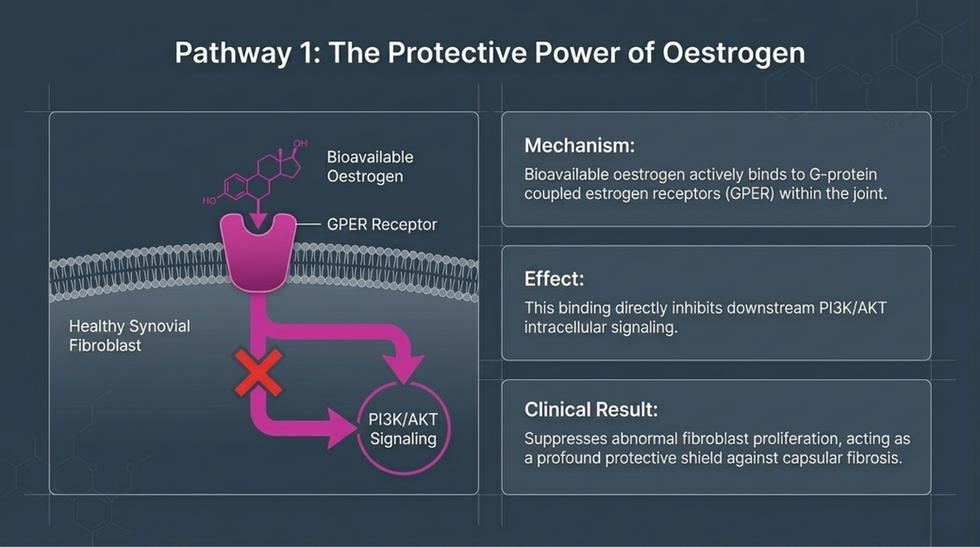
Mechanistically, experimental studies suggest that oestrogen inhibits PI3K/AKT signalling in synovial fibroblasts, reduces activation and fibrosis, decreases extracellular matrix deposition, and exerts anti-fibrotic effects via G protein-coupled oestrogen receptors (GPER). Oestrogen receptors have been identified in capsule fibroblasts, endothelial cells and synovial lining.
In oestrogen-deficient or oestrogen-resistant states, these protective mechanisms are reduced, promoting fibroblast proliferation, excessive collagen deposition, sustained pro-inflammatory macrophage activity and altered collagen turnover.
Clinical implication: peri- and post-menopausal status, HRT use and symptoms suggestive of oestrogen deficiency should be part of the history, with appropriate medical referral where indicated.
Thyroid Dysfunction

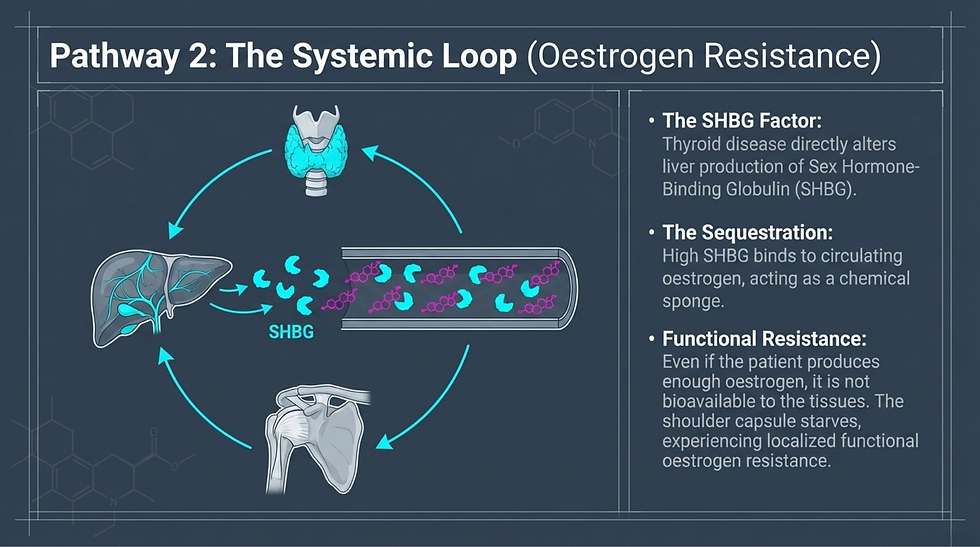
Thyroid disorders are consistently associated with increased frozen shoulder risk. Case-control studies report higher prevalence of hypothyroidism in frozen shoulder cohorts than in controls. Large national cohort data identify hyperthyroidism as an independent risk factor with modestly elevated hazard ratios, and meta-analyses confirm a positive association between thyroid disease — particularly hypothyroidism — and frozen shoulder.
Proposed mechanisms include reduced MMP activity and increased TGF-β favouring extracellular matrix accumulation in the capsule, altered sex hormone-binding globulin (SHBG) reducing oestrogen bioavailability, and induction of insulin and leptin resistance creating a state of functional oestrogen resistance.
Clinical implication: there is growing consensus that thyroid screening is warranted in frozen shoulder, especially when other endocrine or metabolic risk factors are present.
Psychosocial & Neuroendocrine Factors
HPA Axis, Cortisol and ACTH
Expert consensus has identified ACTH deficiency as a potential risk factor, linking frozen shoulder with broader HPA axis dysregulation. Chronic excess cortisol — whether from psychological stress or endocrine disease — may weaken collagen, reduce tissue elasticity and promote capsular fibrosis.
Clinical implication: persistent stress and known HPA axis disorders should inform risk profiling and referral decisions.
Anxiety, Depression and Prognosis
Systematic reviews show that people with frozen shoulder commonly report higher levels of anxiety and depression than healthy controls, and that these factors are associated with worse pain, disability and quality of life.
Higher depression scores correlate with more intense pain and reduced quality of life.
Anxiety is linked to greater upper limb disability and worse pain ratings.
Pain-related fear, depression and pain catastrophising can predict poorer functional outcomes over time.
Current evidence is largely cross-sectional, so it is not yet clear whether psychological distress precedes frozen shoulder or develops as a consequence of persistent pain.
Clinical implication: psychological screening (e.g. HADS, BDI/BAI, PCS) can help identify patients who may be at higher risk of prolonged symptoms or poorer response to treatment.
Emotional Disorders and Frozen Shoulder


Recent cross-sectional work reports that only a small proportion of frozen shoulder patients show no associated emotional disorder. The majority present with anxiety alone, depression alone, or most commonly a combination of both. In some cohorts, the co-occurrence of anxiety and depression shows a strong statistical association with frozen shoulder diagnosis, and outperforms age and sex as a predictor.
Clinical implication: co-existing anxiety and depression should be considered a meaningful part of the clinical picture, not an incidental finding.
Kinesiophobia, Self-Efficacy and Sleep
Kinesiophobia and low pain self-efficacy together can explain a significant portion of the variance in disability and activity-related pain, independent of range-of-motion loss.
Sleep quality in frozen shoulder patients is often poorer than in matched controls, with bidirectional links between sleep disruption and pain sensitivity.
From a neuroimmunological perspective, chronic psychosocial stress and poor sleep activate the HPA axis and sympathetic nervous system, elevating pro-inflammatory cytokines such as IL-1β, IL-6 and TNF-α — mediators also found in frozen shoulder capsular tissue.
Clinical implication: assessment should include kinesiophobia (e.g. TSK-11), pain self-efficacy and sleep (e.g. PSQI), with appropriate psychoeducation and sleep-focused strategies integrated into management.
Metabolic Intersections
Diabetes mellitus and metabolic syndrome are well-established comorbidities of frozen shoulder. Hyperglycaemia promotes the formation of advanced glycation end-products (AGEs), which activate RAGE receptors and downstream NF-κB, increasing pro-inflammatory cytokine expression, stiffening capsular collagen through cross-linking, interfering with cholesterol handling and oestrogen biosynthesis, and downregulating oestrogen receptor expression even when circulating oestrogen is adequate.
Recent retrospective work highlights that female sex, diabetes, poor sleep quality and constipation can act as independent risk factors, with metabolic and lifestyle variables showing stronger associations than purely structural or occupational factors.
Clinical implication: metabolic status (HbA1c, lipids, BMI) and lifestyle factors are integral to assessment and should guide collaborative management with primary care or endocrinology.
Diagnosing Frozen Shoulder: Key Clinical Tests
Understanding the systemic drivers of frozen shoulder is only half the clinical picture. Accurately identifying the condition in the first place requires a structured orthopaedic examination. Adhesive capsulitis is uniquely diagnosed through a combination of severe range-of-motion loss and specific pain provocation tests. The following tests demonstrate the highest diagnostic validity for frozen shoulder.
1. The Coracoid Pain Test
The Coracoid Pain Test has one of the highest validity scores for frozen shoulder, with studies reporting both specificity and sensitivity above 96%. The examiner palpates the coracoid process and the acromioclavicular (AC) joint. The test is positive when pain is significantly more severe at the coracoid than at the AC joint and anterolateral subacromial area.
For the highest diagnostic certainty, clinicians typically combine a capsular pattern of restriction — external rotation being the most limited, followed by abduction and then internal rotation — with a positive Coracoid Pain Test.
2. The Shoulder Shrug Sign
Highly sensitive (often above 95%) for detecting a stiff shoulder, the Shoulder Shrug Sign is observed during active bilateral arm abduction to 90 degrees. A positive sign is present when the patient elevates the entire scapula and shoulder girdle to lift the arm, compensating for restricted glenohumeral movement. It is worth noting that advanced rotator cuff tears and osteoarthritis can also produce a positive sign, so it should not be used in isolation.
3. Passive External Rotation Restriction
While not a named orthopaedic test, the measurement of passive external rotation is considered the clinical gold standard and carries the highest diagnostic validity for early-stage frozen shoulder. With the elbow stabilised at the side (0 degrees of abduction), the examiner passively externally rotates the arm. A definitive, firm and painful mechanical block with a capsular end-feel — typically limiting external rotation to less than 30 degrees, or at least 50% loss compared to the unaffected shoulder — constitutes a positive finding.
4. Apley's Scratch Test
Apley's Scratch Test offers excellent reliability and moderate validity for tracking the progression and capsular pattern of adhesive capsulitis. The patient attempts to touch the opposite scapula in two directions: reaching behind the head (testing abduction and external rotation) and reaching behind the back (testing adduction and internal rotation). A severe and asymmetrical inability to reach the landmarks compared to the unaffected shoulder constitutes a positive result.
An Integrated Model
An emerging biopsychosocial-hormonal model proposes that frozen shoulder reflects the convergence of four overlapping systems:
Hormonal vulnerability (menopause, thyroid disorders, HPA axis dysregulation) creating a pro-fibrotic, pro-inflammatory capsular environment.
Psychosocial stress, anxiety, depression and sleep disruption amplifying HPA activity, altering oestrogen receptor sensitivity and driving central sensitisation.
Metabolic disruption (hyperglycaemia, AGEs, dyslipidaemia) impairing oestrogen biosynthesis and signalling while stiffening collagen.
Local capsular changes interacting with these systemic influences to produce the familiar clinical picture of pain, stiffness and prolonged recovery.
This framework helps explain why frozen shoulder disproportionately affects peri- and post-menopausal women, why psychological comorbidity is so frequent, and why outcomes often correlate more closely with psychosocial and metabolic measures than with range-of-motion alone.
Clinical Takeaways for Physiotherapy


For day-to-day practice, this evidence supports:
Routine screening for anxiety, depression, sleep quality, kinesiophobia and pain catastrophising.
Considering endocrine and metabolic referral (thyroid panel, oestradiol, HbA1c) where risk factors or symptoms are present.
Integrating pain neuroscience education and graded exposure to address fear-avoidance and low self-efficacy.
Liaising with GPs around possible HRT discussion in suitable peri-/post-menopausal women.
Using biopsychosocial outcome measures alongside ROM to monitor progress.
A whole-person approach that recognises hormonal, metabolic and psychosocial influences may better reflect the true nature of frozen shoulder and offer more targeted, effective care.
Frozen Shoulder Treatment at Functional Body Clinic, Birmingham
If you are experiencing persistent shoulder stiffness, night pain or restricted range of motion, Functional Body Clinic can help. Frozen shoulder is not simply a mechanical problem in an isolated joint — as this evidence review makes clear, it is a multifactorial condition rooted in hormonal vulnerability, metabolic disruption and psychosocial stress. Treating only the local tissue without addressing these wider drivers is one of the key reasons many people find their recovery slower or less complete than expected.
At Functional Body Clinic, assessment goes beyond measuring range of motion. Using validated orthopaedic shoulder tests — including the Coracoid Pain Test, passive external rotation assessment and Apley’s Scratch Test — alongside a thorough biopsychosocial history, every consultation considers the hormonal, metabolic and psychosocial factors that may be fueling your symptoms. This whole-person approach forms the foundation of a targeted, evidence-informed management plan that works with your body’s biology rather than against it.
To book your shoulder assessment at Functional Body Clinic in Birmingham, click here to book. Taking the first step towards understanding what is truly driving your shoulder pain could make all the difference to your recovery.

Further reading & next steps
If this article rang uncomfortably true for your sport or your job, these pieces go deeper into how we assess and treat those loading patterns at Functional Body Clinic:
The Benefits of Maintenance Massage: Keeping Your Body in Peak Condition – how regular treatment helps tissues adapt instead of fail under repetitive stress.
What is Maintenance Massage and Why Should You Consider It? – when to move from crisis‑only treatment to a planned maintenance approach.
And if you already know your body is paying the price for your sport or work, you can explore our care plans and book an assessment:
Sports Massage Plan – Birmingham – for athletes and “industrial athletes” who need performance and recovery support.
Holistic Deep Tissue Plan – for long‑standing stiffness, recurrent pain, and postural overload.
Care Plans – structured treatment plans for ongoing spinal, shoulder, and hip issues.



Comments