
The Price of Excellence: Understanding Injury Risks in Sports and Work
- Adrian Wildborne

- Apr 24
- 12 min read
Updated: May 4
There is a particular cruelty to the way elite careers end. Not in a blaze of competitive glory, but in a surgeon's consulting room. A spinal disc that can no longer bear the load. A hip joint ground down to bone-on-bone. A knee that has absorbed five million landings too many. When it happens, the narrative is almost always the same: "He just landed awkwardly," "It was a freak twist," "Nobody could have seen it coming."
But here is what the biomechanics literature is telling us with increasing clarity: they almost always could have. The "freak accident" is, in the vast majority of cases, the final legible entry in a ledger that has been accumulating for years — sometimes decades. The body does not break randomly. It breaks mathematically. If we could learn to read that ledger in real time, rather than in the post-mortem, we would be sitting at the frontier of the most important shift in sports medicine and soft tissue therapy in a generation.
The Body Is Not a Machine — It Is Something More Dangerous
We often describe the human body using mechanical metaphors like levers and pulleys. However, this framing underestimates it in one critical way: a machine wears down passively. The body wears down adaptively. It actively remodels itself to survive the demands placed upon it. In doing so, it sculpts itself into a system that is exquisitely optimised for one thing and quietly catastrophic for everything else.
The scientific framework that captures this most precisely is the concept of the body as a tensegrity structure. Unlike a conventional stack of load-bearing parts, the skeleton does not simply sit atop itself. It floats within a continuous, dynamically tensioned web of myofascial tissue — fascia, muscle, tendon, ligament — where every part influences every other part. Alter the tension in one corner of this web, and you alter the load distribution everywhere else. There is no truly local injury. There is only the place where the system finally declared it could not compensate any further.
The consequence of this architecture, in the context of elite sport, is both profound and underappreciated. When an athlete specialises, they do not simply get better at their sport. They are physically restructured by it. Their fascia remodels along specific loading vectors. Their bone density redistributes asymmetrically. Their muscles lose sarcomeres in chronically shortened positions. Their joints develop morphological changes permanently locked in by skeletal maturity. All of this is perfectly, mechanistically predictable — if you know what to look for.
The 70% Problem Nobody Is Talking About




Before we delve into the mechanisms, let's address the epidemiology plainly. Single-sport specialised athletes are approximately 70% more likely to suffer repetitive overuse injuries than their multi-sport counterparts. Specialised individual sport athletes — gymnasts, dancers, tennis players — experience serious overuse injuries at rates 2.38 times higher than peers who diversified. Athletes who specialise before the age of twelve show burnout rates 3.76 times higher than those who delay until after fifteen.
Perhaps most striking is that the long-term structural consequences of early specialisation do not disappear when the athlete leaves sport. Longitudinal data from US military service academies shows that female cadets with a history of high sport specialisation were 4.25 times more likely to sustain a lower extremity stress fracture in their first year of service than those with low specialisation — long after they had stopped competing. The body remembers. The architectural legacy of the loading pattern persists.
Yet, the cultural infrastructure of elite sport continues to push earlier specialisation, higher training volumes, and year-round intensity. The financial reward structures of professional sport make it almost impossible for athletes or their families to do otherwise. The question is not whether the system is broken. The question is whether we can do better science inside it.
Three Bodies. Three Sports. Three Completely Predictable Breakdowns.
The career injury arcs of three celebrated athletes illustrate this with uncomfortable precision: Michael Jordan, Tiger Woods, and Andy Murray. Three different sports. Three different failure modes. In each case, the specific tissue that failed was almost exactly what you would predict if you simply looked at the dominant loading vectors of the sport.
Michael Jordan: The Compressive Cascade

Basketball is fundamentally a sport of vertical ground reaction forces. Landing from a jump shot generates peak forces of approximately 5.57 times body weight. In the chaotic physics of an actual game, where players land off-balance, fatigued, or colliding with opponents, those forces spike considerably higher. The structure that paid the price in Jordan's case was the tarsal navicular — a small keystone bone in the midfoot arch that is simultaneously the most mechanically loaded bone in the foot and one of the most poorly vascularised. It sits at a biomechanical crossroads where the fulcrum action of the arch concentrates maximum shear and compressive stress in the central third of the bone — a region where blood supply is so limited that repair mechanisms cannot keep pace with even moderate microtrauma accumulation.
Jordan fractured his navicular in October 1985. It was described as an awkward landing. It was not awkward. It was the mathematically inevitable result of thousands of high-impact landings on a vascular watershed zone with insufficient recovery. What saved his career was his background: Jordan had played baseball and football extensively throughout adolescence. This multi-sport development spared his skeletal architecture from the relentless concentration of basketball-specific stress during its most vulnerable developmental window. His diverse foundation bought him years — and his career is as much a vindication of varied athletic development as it is a testament to individual talent.
Tiger Woods: The Rotational Demolition
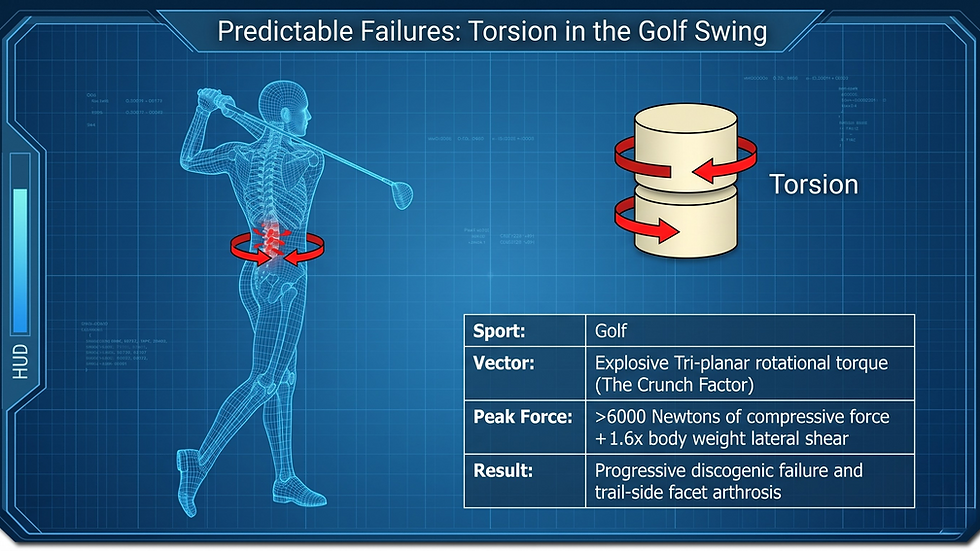
If Jordan's story is about compression, Woods' is about something more insidious: the self-inflicted destruction caused by generating maximum torque against a system that was not built to absorb it indefinitely. The modern golf swing is built around the X-factor: the deliberate restriction of pelvic rotation during the backswing while the thorax achieves up to 110 degrees of rotation. This creates enormous stored elastic energy and lumbar spine forces of six to eight times body weight in compression at the L4-L5 segment, combined with extreme lateral flexion and hyperextension in what biomechanists call the "crunch factor."
Woods began golfing at age two. His skeleton was subjected to tens of thousands of cycles of this asymmetric, high-torque movement before it reached maturity. The failure sequence was entirely predictable: the lead knee gave first, progressing from ACL rupture through cartilage surgery to two simultaneous tibial stress fractures. As the altered kinematics of the reconstructed knee shifted load elsewhere, the lumbar spine absorbed forces it was never designed to sustain, leading to multiple microdiscectomies, spinal fusion, adjacent segment disease, and disc replacement. This is not a series of unfortunate accidents. It is a sequential kinetic chain collapse — the mathematically inevitable progression of structural compromise propagating through an interconnected tensegrity system.
Andy Murray: The Shear and Friction Trap

Andy Murray's hip is perhaps the most clinically instructive case because the mechanism is so precisely traceable to a single biomechanical demand. Modern hard-court tennis requires abrupt deceleration on high-friction surfaces, combined with the extreme hip positions of the open-stance groundstroke. The Defensive Open Stance forces the hip into simultaneous maximal flexion, extreme abduction, and severe external rotation, generating massive anterior and medial forces on the joint while creating intense shear on the acetabular labrum.
Murray's underlying structural vulnerability was Femoroacetabular Impingement (FAI) — a morphological condition that, in a sedentary person, may never cause symptoms. Combined with millions of high-friction pivots on hard courts through intensive adolescent training, the bony abnormalities repeatedly crushed and tore the fibrocartilaginous labrum. Once that vital suction seal was compromised, the cartilage was literally ground away. By 2019, he could not put on socks without agonising pain. He required a Birmingham Hip Resurfacing — a metal-on-metal joint specifically engineered to tolerate the shear vectors that his biological cartilage could no longer absorb. The tissue that failed was entirely predictable from the loading vectors of the sport. It is not a mystery. It is a biomechanical equation.
What Is Actually Happening in the Tissue

To understand why these failures are predictable — and more importantly, why they can be deferred or mitigated — it helps to understand the biological cascade that precedes them. It begins with fascial densification. The myofascial matrix relies on hyaluronic acid (HA) to maintain the frictionless slide and glide between adjacent tissue layers. In healthy, dynamically varied movement, HA behaves as a thixotropic fluid: it stays mobile, lubricating the interfaces between muscle fascicles, fascial planes, and joint structures.
When tissue is chronically subjected to identical, narrow loading patterns — the same rotation, the same compressive vector, the same eccentric deceleration, repeated tens of thousands of times — HA begins to aggregate into dense, high-molecular-weight structures that shift the ground substance toward something closer to viscous gel. Adjacent fascial layers that should slide freely begin to adhere. This acute densification develops within minutes to hours and is reversible with movement, shear, and heat. But left unaddressed, it initiates a cascade with far longer timelines.
Within two to four weeks of sustained shortening, muscles begin to delete serial sarcomeres — losing between 20% and 40% of their contractile units in series. The tissue becomes structurally shorter: mechanically robust within its new, abbreviated range, but catastrophically vulnerable if a dynamic athletic movement demands its full historical length. At the six to twelve month mark, fibroblasts differentiate into myofibroblasts — cells that lay down dense, disorganised collagen along the exact lines of repetitive stress, transitioning the tissue from functional densification into chronic, plastic fibrosis with recovery timelines of six to twenty-four months.
The Structural Vulnerability Window

Cartilage takes ten to twelve weeks to meaningfully adapt to new loads. Muscle takes two to four weeks. The athlete's subjective readiness returns in weeks. However, the passive joint structures are still structurally compromised months later. This mismatch creates what biomechanists call the structural vulnerability window — the period in which an athlete feels capable of full intensity but their passive tissues have not yet caught up. Catastrophic joint failures and severe tendinopathies typically occur four to eight weeks after the initial load spike has already passed. Feeling ready is not the same as being structurally prepared.
The Industrial Athlete: When Your Job Is the Sport

Everything described above applies with equal force to the occupational environment. Human tissue does not differentiate between the pursuit of a Grand Slam and a twelve-hour surgical shift. The Kinesiopathologic Model — the principle that repetitive, specialised movement patterns are themselves the primary vector of pathology — operates identically in a warehouse, an operating theatre, or a professional golf tour.
Consider the shoulder. A professional tennis player develops subacromial impingement and rotator cuff failure through high-velocity eccentric deceleration. The posterior cuff absorbs massive braking forces after every serve, while the posterior capsule progressively fibroting into glenohumeral internal rotation deficit (GIRD), producing SLAP tears. A consultant surgeon develops the same endpoint through prolonged static overload. Hovering over an operating table, when a surgical instrument is held 50cm from the glenohumeral joint, the supraspinatus must generate sustained isometric forces twenty times greater than the weight of the instrument simply to maintain stability. The sustained capillary occlusion initiates hyaluronic acid aggregation in the subacromial gliding planes, narrowing the subacromial space — producing the same endpoint: rotator cuff tears, bursitis, and C5-C7 disc herniations. Different mechanism. Same anatomical destination.
The same parallel holds for the lumbar spine. Professional golfers develop progressive discogenic failure through explosive tri-planar torque generating over six thousand Newtons of compressive force at L4-L5. Warehouse operatives develop the same endpoint through repetitive asymmetric lifting that routinely exceeds the fatigue failure threshold for lumbar shear, combined with hours of sustained spinal flexion driving viscoelastic creep. This is where the passive fascial springs of the thoracolumbar fascia gradually lose their elasticity and cease to provide intrinsic trunk stiffness. The golfer generates the damage explosively over a long career. The warehouse operative generates it cumulatively, minute by minute. The endpoints are functionally identical.
The Current Clinical Failure: Treating the Symptom, Ignoring the Signature
Here is where the existing model breaks down. A golfer presents with right-sided lower back pain. They receive a diagnosis of lumbar disc herniation. Treatment is directed at the disc. However, the underlying loading signature that created the herniation — the restricted lead hip internal rotation forcing compensatory lumbar hyper-rotation, the asymmetric X-factor torque of the modern swing, the locked-short deep multifidus and oblique slings — is not assessed, treated, or modified. The golfer returns to playing, but the loading signature continues unchanged. The system fails again, often at a higher level.
This pattern repeats across virtually every overuse presentation in sport and occupational health. The tissue is treated in isolation. The mechanical context that created the tissue failure — the patient's specific wear signature, the repetitive loading vectors of their sport or occupation, the myofascial slings that are locked short, and the fascial densifications forcing compensatory load elsewhere — is left entirely unaddressed. It is the equivalent of repeatedly replacing a burned-out lightbulb without examining the wiring.
A Different Framework: Load Phenotyping
What the research is pointing toward is a fundamental shift in how we approach both athletic injury prevention and occupational musculoskeletal health. Rather than treating pathology after it declares itself, the clinical priority should be identifying the patient's load phenotype — the specific mechanical dietary habits of their daily sport or work — and intervening at the level of the pattern, before the tissue reaches its failure threshold.
This means asking different questions before treatment begins. What are the dominant loading vectors of this person's sport or occupation? Is the primary stress compressive, rotational, or shear-based? Which myofascial slings are likely locked-short? Where in the kinetic chain is the "victim" joint compensating for a restricted "slacker" joint elsewhere? The goal is not to eliminate the specialised loading — we cannot stop the golfer from golfing or the surgeon from operating. The goal is to prevent adaptive maladaptation: the progressive loss of tissue compliance in off-axis directions that leaves the body unable to absorb the unpredictable forces of competition or occupational fatigue without failing.
In practice, this means identifying and addressing fascial densification before it becomes fibrosis. The window between acute, reversible densification and chronic plastic remodelling is real and clinically meaningful. Targeted manual therapy utilising tangential shear can mechanically liquefy densified hyaluronic acid matrices and restore fascial glide. It also means restoring sarcomere number in chronically shortened tissues through loaded eccentric work and restoring multiplanar tissue compliance. Fascia exposed exclusively to one loading vector for years becomes brittle in all others.
What This Means Beyond the Clinic
The prevailing model of elite athletic development is still essentially Faustian: sacrifice your long-term physical architecture on the altar of short-term performance. Specialise early, train hard, and if your body eventually fails, that is the price of excellence. However, the biomechanics literature increasingly suggests this trade-off is not inevitable — it is just underinformed.
Michael Jordan's multi-sport background is not a biographical curiosity. It is a controlled variable in a natural experiment. His diverse mechanical loading during skeletal development distributed stress across varied kinetic chains, prevented the extreme asymmetric remodelling of the early specialiser, and built a proprioceptive repertoire that allowed him to dissipate ground reaction forces more efficiently throughout his career. The late specialiser is not developmentally disadvantaged. In the majority of athletic disciplines, the evidence suggests the opposite: the early specialiser accumulates mechanical debt faster, burns out sooner, and carries a structural legacy that limits long-term competitive longevity.
For the occupational population — surgeons, warehouse operatives, manufacturing workers, tradespeople — the argument is even more urgent. Work-related musculoskeletal disorders carry a total economic burden approaching £849 billion in the United States alone. These populations rarely have access to the biomechanical assessment frameworks available to professional athletes. They present with a painful shoulder or a herniated disc and receive symptomatic treatment that sends them back to the exact loading environment that created the problem, unchanged. This is a solvable problem. The tools exist. What has historically been missing is the integration of sports biomechanics thinking into the occupational and clinical context.
The Ledger Is Always Running
Your body is keeping a rigorous mathematical ledger of your movements. Every repetition you perform — every serve, every swing, every lift, every hour spent hovering over an operating table — is entered into that ledger. The tissue adapts, the fascia remodels, the bone reshapes, and the sarcomeres are added or deleted. The body does not forget a single entry.
What elite soft tissue therapy can do is read that ledger proactively, before the tissue reaches its failure threshold. Identify the specific loading signature. Find the myofascial slings that are locked-short, the joints that are being asked to compensate for restrictions elsewhere, and the fascial matrices that are beginning to densify. Intervene with enough precision and lead time to prevent the predictable from becoming inevitable.
The Price of Excellence: Reducing the Risk
This is not about erasing the miles an athlete has covered or asking a warehouse operative to work differently than their job demands. It is about understanding the specific mechanical forces going through specific tissues, at the level of resolution those forces deserve. Use that understanding to keep the vehicle running — rather than waiting for it to break down on the same corner every time. The capacity to predict is the capacity to prevent. If the research in this field tells us anything, it is that we have far more capacity to predict than we are currently using.

Further reading & next steps
If this article rang uncomfortably true for your sport or your job, these pieces go deeper into how we assess and treat those loading patterns at Functional Body Clinic:
The Benefits of Maintenance Massage: Keeping Your Body in Peak Condition – how regular treatment helps tissues adapt instead of fail under repetitive stress.
What is Maintenance Massage and Why Should You Consider It? – when to move from crisis‑only treatment to a planned maintenance approach.
And if you already know your body is paying the price for your sport or work, you can explore our care plans and book an assessment:
Sports Massage Plan – Birmingham – for athletes and “industrial athletes” who need performance and recovery support.
Holistic Deep Tissue Plan – for long‑standing stiffness, recurrent pain, and postural overload.
Care Plans – structured treatment plans for ongoing spinal, shoulder, and hip issues.


Comments